HIV Infection Stage Tracker
Stages of HIV infection:
- Acute Infection: 2-4 weeks post-exposure
- Clinical Latency: Years of low-level replication
- AIDS: CD4 count below 200 cells/µL
Acute Infection: Occurs 2-4 weeks after exposure. Symptoms resemble flu. High viral load.
Clinical Latency: Virus remains active but reproduces at low levels. Often asymptomatic. CD4 count gradually declines.
AIDS: Defined by CD4 count below 200 cells/µL or presence of opportunistic infections.
With proper antiretroviral therapy (ART), many people never progress to AIDS.
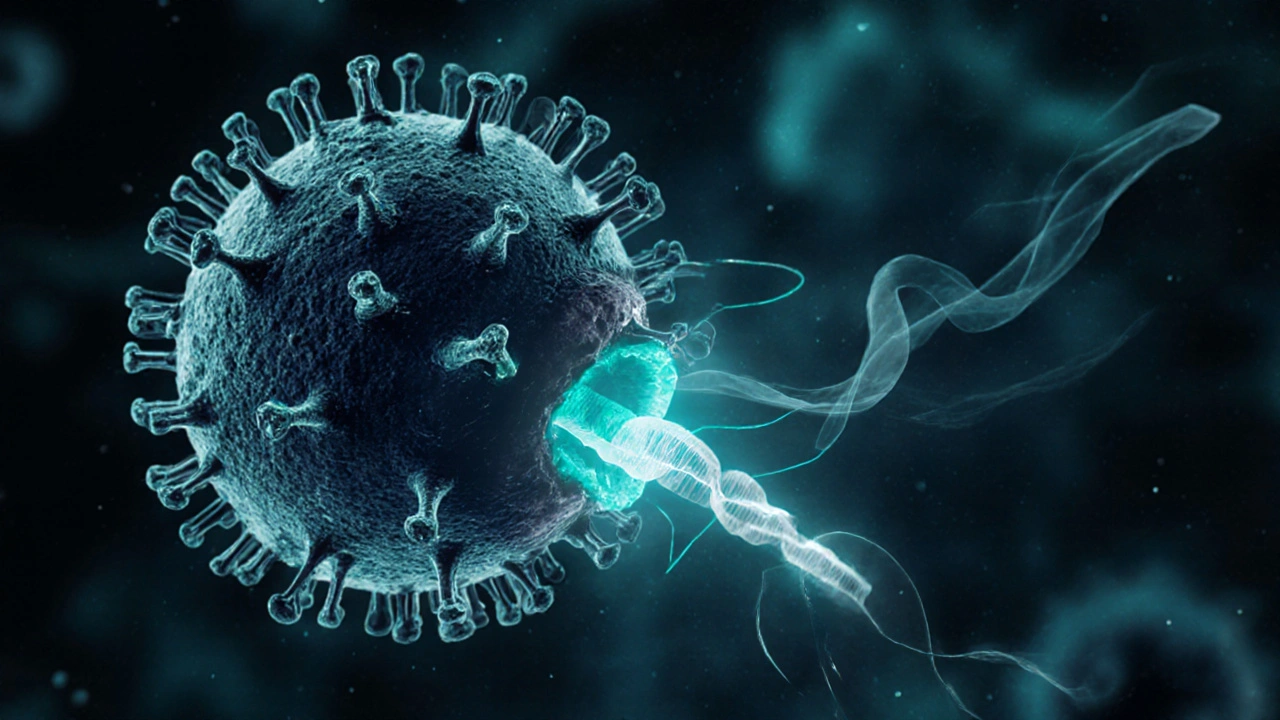
When the first cases of AIDS appeared in the early 1980s, scientists were baffled by a mysterious HIV a retrovirus that attacks the human immune system. Today more than 38 million people worldwide live with the virus, and understanding how it works is key to controlling the epidemic.
HIV is not just a medical term; it represents a complex battle inside every infected body.
What is HIV and How Does It Replicate?
AIDS the advanced stage of HIV infection when the immune system can no longer defend against opportunistic infections begins with the virus entering a host cell. HIV is a lentivirus, a subgroup of retroviruses that can integrate its genetic material into the DNA of the cell it infects. Once inside, the virus uses an enzyme called reverse transcriptase to copy its RNA genome into DNA, which then inserts into the host’s genome.
This integration lets HIV hijack the cell’s machinery to churn out new viral particles. Every 9 to 12 hours, an infected cell can release thousands of new virions, spreading the infection throughout the body.
The Immune System Targets of HIV
The primary victims are a type of white blood cell called CD4 T cells a subset of lymphocytes that coordinate immune responses. HIV binds to the CD4 receptor and a co‑receptor (typically CCR5 or CXCR4) to gain entry. As the virus replicates, the number of functional CD4 T cells drops, weakening the immune response.
Other immune cells, such as macrophages and dendritic cells, also serve as reservoirs where the virus can hide from the immune system and from many drugs. This hidden pool makes eradication extremely challenging.
Stages of HIV Infection
- Acute infection - Occurs 2‑4 weeks after exposure. Flu‑like symptoms appear as the virus multiplies rapidly.
- Clinical latency - Virus remains active but reproduces at lower levels. People often feel healthy while CD4 counts slowly decline.
- AIDS - Defined by a CD4 count below 200 cells/µL or the presence of opportunistic infections.
The length of each stage varies; with modern treatment, many people never progress to AIDS.
Measuring Viral Load and Monitoring Progress
Viral load the quantity of HIV RNA copies per milliliter of blood is the most direct indicator of how actively the virus is replicating. A high viral load correlates with faster CD4 decline and greater transmission risk.
Regular testing-typically every three to six months-helps clinicians adjust therapy before the immune system is severely compromised.
Antiretroviral Therapy (ART) - How It Works
Antiretroviral therapy a combination of drugs that block different stages of the HIV life cycle is the cornerstone of modern HIV care. The most common regimen includes:
- Two nucleoside reverse‑transcriptase inhibitors (NRTIs) that mimic building blocks of viral DNA, causing premature termination.
- One integrase strand transfer inhibitor (INSTI) that prevents the viral DNA from integrating into the host genome.
- Optionally, a non‑nucleoside reverse‑transcriptase inhibitor (NNRTI) or a protease inhibitor (PI) for added potency.
When taken consistently, ART suppresses viral load to undetectable levels-usually under 20 copies/mL. At this point, the virus cannot be sexually transmitted, a concept known as U=U (Undetectable = Untransmittable).
HIV‑1 vs HIV‑2: A Quick Comparison
| Attribute | HIV‑1 | HIV‑2 |
|---|---|---|
| Global prevalence | ≈ 95% of infections | ≈ 1-2% of infections, concentrated in West Africa |
| Transmission efficiency | Higher; easier via sexual contact, blood | Lower; requires higher viral load for transmission |
| Progression to AIDS | Usually within 10 years without treatment | Often slower; many remain asymptomatic longer |
| Response to ART | Well‑studied, standard regimens effective | Requires specific drugs; some NRTIs less effective |
| Diagnostic tests | Standard antibody/antigen kits detect | Some kits miss HIV‑2; need specialized PCR |
Vaccine and Cure Research: What’s on the Horizon?
Despite decades of effort, no licensed HIV vaccine exists yet. Current strategies fall into three categories:
- Broadly neutralising antibodies (bNAbs) - Lab‑engineered antibodies that target conserved regions of the virus.
- Vector‑based vaccines - Use harmless viruses to deliver HIV genes, prompting an immune response.
- mRNA platforms - Inspired by COVID‑19 vaccines, they encode HIV envelope proteins.
Clinical trials in 2024 showed that a combination of mRNA‑encoded bNAbs provided temporary protection in a small cohort, a promising sign for future larger studies.
On the cure front, two approaches dominate:
- “Kick‑and‑kill” - Reactivate latent virus reservoirs and then eliminate infected cells with immune‑based therapies.
- Gene editing - CRISPR‑Cas systems aim to excise proviral DNA from host chromosomes.
While no cure is clinically available, the “Berlin patient” case-where a bone‑marrow transplant from a donor with a natural CCR5 mutation cured HIV-provides a proof‑of‑concept that a functional cure is biologically possible.
Everyday Strategies to Stay Healthy with HIV
Living with HIV today is manageable, but success hinges on a few practical habits:
- Adhere to ART without missed doses; set reminders or use a pill‑box.
- Get viral load and CD4 count checks regularly; ask your clinician about resistance testing if viral load climbs.
- Maintain a balanced diet rich in fruits, vegetables, and lean protein to support immune recovery.
- Exercise moderately-30 minutes most days improves cardiovascular health and metabolic markers.
- Vaccinate against hepatitis B, HPV, flu, and COVID‑19; these infections can strain an already weakened immune system.
Community support groups, especially those online, also boost mental health, which correlates with better treatment outcomes.
Frequently Asked Questions
Can an HIV‑positive person lead a normal life?
Yes. With consistent antiretroviral therapy, most people achieve undetectable viral loads, enjoy normal lifespans, and have a quality of life comparable to uninfected individuals.
What does ‘undetectable’ really mean?
Undetectable means the viral load is below the test’s threshold-typically under 20 copies per millilitre. At this level, the virus cannot be transmitted sexually, and the immune system is protected from damage.
Why does HIV have so many subtypes?
HIV is an RNA virus with a high mutation rate. Each replication cycle introduces errors, creating diverse strains. This genetic diversity helps the virus evade immune responses and complicates vaccine design.
Is there any risk of contracting HIV from casual contact?
No. HIV cannot survive outside the body for long and does not spread through air, water, sharing utensils, or casual touch. Transmission requires exchange of certain bodily fluids, such as blood, semen, vaginal secretions, or breast milk.
What are the biggest challenges in finding an HIV cure?
The virus hides in latent reservoirs-cells where it integrates DNA but remains dormant. These cells can survive for years, evading both the immune system and drugs. Eliminating or permanently silencing these reservoirs is the central hurdle for a cure.



Wow, this article really breaks down the HIV life cycle in a way that’s easy to digest. It's fascinating how the virus hijacks reverse transcriptase to turn its RNA into DNA, then slips that into our genome. The detail on CD4 T‑cell depletion really helps illustrate why the immune system collapses. Also, the part about antiretroviral therapy keeping viral loads undetectable gives a lot of hope for people living with HIV.
Just a minor note: the article writes "viral load the quantity of HIV RNA copies" – it should be "viral load is the quantity of HIV RNA copies".
Dear readers, the comprehensive overview presented herein is both scientifically accurate and compassionately written. It is commendable how the piece elucidates the mechanisms of reverse transcription with clarity. The discussion of ART regimens reflects current best practices. Moreover, the emphasis on regular monitoring aligns with standard clinical guidelines. I trust that many will find this information reassuring and empowering.
The article is an exemplary synthesis of virology and public health.
This is why America must stay vigilant against foreign viruses that threaten our citizens. We need stronger borders and more funding for domestic biotech. Only then can we safeguard our freedoms.
While vigilance is important, it's also crucial to support those already affected by HIV with compassion and resources. Stigma only hinders progress. Let's focus on education and treatment access.
Ah, the elegant choreography of a virus that, in its ruthless efficiency, mirrors the very entropy we observe in the cosmos; every step of its replication a reminder of the delicate balance between order and chaos!; yet, behold the sheer audacity of reverse transcriptase, forging DNA from RNA as if defying the Second Law of Thermodynamics itself-truly a molecular marvel!; the integration of proviral DNA into host chromosomes is akin to a clandestine spy embedding itself within a foreign embassy; it whispers, "I am one of you," while plotting subversion.
Consider the CD4+ T‑cells: the conductors of our immune symphony, now silenced one by one, reducing the amplitude of our defenses; it is as if a maestro's baton is removed mid‑performance, leaving discord in the hall.
Enter antiretroviral therapy-our modern shield-targeting distinct stages of this viral opera with nucleoside analogues, integrase inhibitors, and protease blockers; each drug a note in a counter‑melody that strives to restore harmony.
The concept of undetectable = untransmittable (U=U) is not just a medical milestone but a sociocultural proclamation: stigmas crumble when viral loads drop below 20 copies/mL, turning fear into empowerment! 😊
Yet, the persistence of latent reservoirs-macrophages, dendritic cells-poses an epistemic puzzle, a Schrödinger’s cat of virology: invisible, dormant, yet ever‑present.
Vaccine research, with its broad‑neutralising antibodies and mRNA platforms, seeks a prophylactic bulwark, a preemptive strike against the virus's incursion, echoing the ancient art of siege defense.
On the cure frontier, the “kick‑and‑kill” and CRISPR‑Cas strategies attempt to purge these hidden sanctuaries, reminiscent of a meticulous gardener removing weeds before they overrun the garden.
From a philosophical lens, HIV challenges our notions of identity, as the virus blurs the line between self and other, prompting us to ask: what does it mean to be “infected” when the invader becomes part of our genomic narrative?
In sum, the science of HIV is a tapestry woven from molecular biology, clinical practice, and human experience; each thread essential, each hue vivid, each pattern instructive.
Great philosophical breakdown! It really drives home how complex the battle against HIV is. Keeping up with ART and regular check‑ups is the most practical step we can all take.
Minor typo spotted: "HIV‑1 vs HIV‑2: A Quick Comparison" should have "A" capitalized for consistency. Also, "CD4 count below 200 cells/µL" could be clarified as "CD4 count falling below 200 cells per microliter".
Keep fighting the good fight! 💪
Isn't it suspicious how quickly the "cure" narrative shifts each election cycle? The pharma lobby must be pulling strings behind the scenes. I swear the same headlines keep resurfacing, just with different buzzwords.
While skepticism can be healthy, spreading unfounded theories only fuels stigma and hinders real progress. People living with HIV deserve accurate information and support, not fear‑mongering.
From my experience in infectious disease research, the latency reservoir is the primary obstacle to eradication. Even with potent ART, integrated proviral DNA persists in resting CD4+ T cells and myeloid compartments. Recent CRISPR attempts show promise but off‑target effects remain a critical concern. Additionally, the genetic diversity of HIV‑1 subtypes complicates vaccine design, as epitopes vary substantially across clades. Therefore, a multi‑pronged approach integrating latency reversal agents, immune modulation, and gene editing is likely required for any functional cure.
All this talk about global solutions forgets that America must lead the charge. Our biotech industry has the resources to dominate the cure race, and we should prioritize funding here. International collaboration is fine, but don't let foreign interests dictate our agenda.