
When you’re managing asthma, inhaled corticosteroids (ICS) are often the most effective tool you have. They calm inflammation in your airways, prevent flare-ups, and help you breathe easier day after day. But if you’ve been using them for months or years, you might have noticed a hoarse voice, a fungal infection in your mouth, or unexplained bruising. These aren’t just minor annoyances-they’re real side effects, and they’re more common than most people realize.
The good news? Most of these side effects are preventable. And the risk isn’t the same for everyone. It depends on the type of steroid you’re using, how much you’re taking, and whether you’re using it correctly. The key isn’t to stop your medication-it’s to use it smarter.
What Are the Most Common Side Effects of Asthma Steroids?
Side effects from inhaled steroids fall into two categories: local and systemic. Local effects happen right where the medicine lands-your mouth and throat. Systemic effects happen when a small amount gets into your bloodstream and affects your whole body.
For local side effects, the top three are:
- Oral thrush (a yeast infection in the mouth): Affects up to 42% of users, especially those who don’t rinse after inhaling.
- Hoarse voice or dysphonia: Happens in about 38% of people, often because the steroid sticks to the vocal cords.
- Throat irritation or coughing: Reported by over 30% of users, usually due to poor inhaler technique.
Systemic side effects are less common but more serious. They include:
- Adrenal suppression: Your body stops making its own cortisol if you’re on high doses long-term. Fluticasone at 500 mcg/day or more carries nearly 3 times the risk of this compared to budesonide.
- Skin thinning and bruising: Especially in older adults. One study found 34% of people on high-dose ICS for over five years had noticeable skin changes.
- Bone density loss: Risk increases after 5 years on doses above 750 mcg/day of beclomethasone equivalent.
- Pneumonia: For people over 65, high-dose ICS raises the risk by nearly 70% compared to low doses.
It’s not a lottery-these effects are predictable. And they’re dose-dependent. The higher your daily dose, the greater your risk. But many people don’t realize they’re on more than they need.
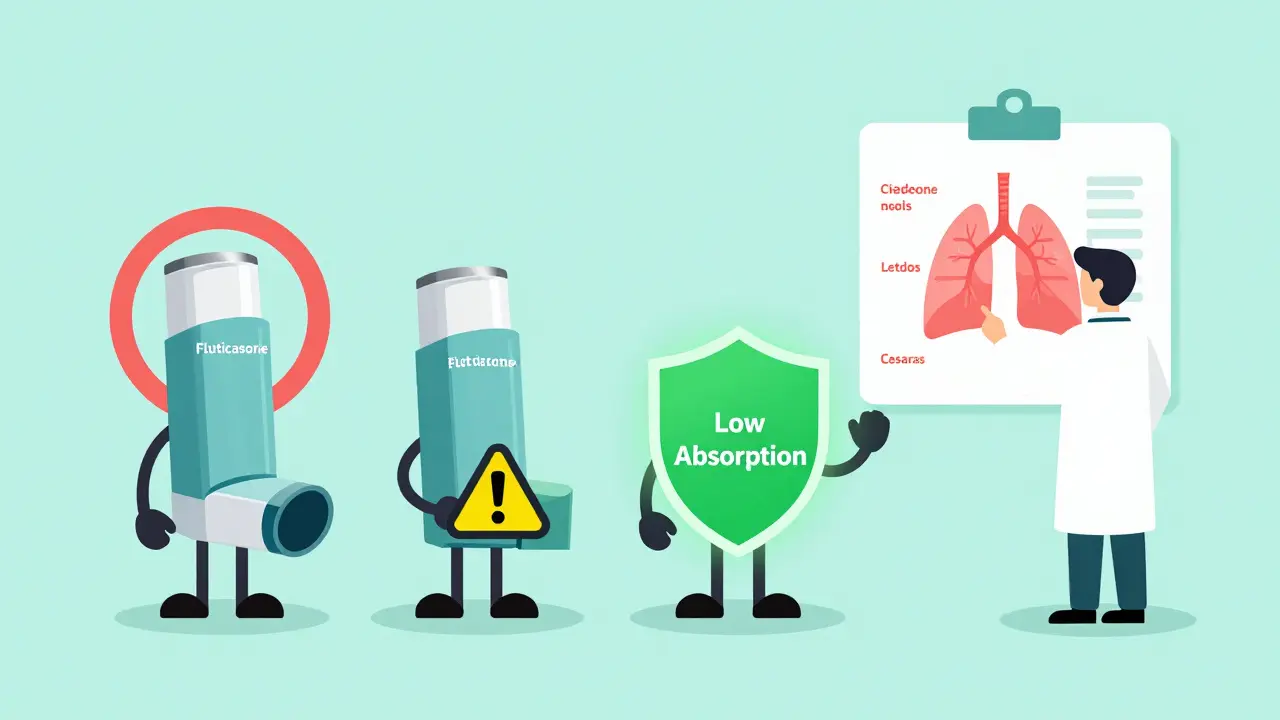
Not All Steroid Inhalers Are the Same
If you think all inhalers are created equal, you’re not alone. But they’re not. Different steroids have different absorption rates, and that makes a big difference in side effects.
Here’s how they stack up:
| Medication | Systemic Absorption | Typical Daily Dose Range | Relative Risk of Adrenal Suppression |
|---|---|---|---|
| Fluticasone propionate | 30-40% | 100-500 mcg | High |
| Budesonide | 10-15% | 200-800 mcg | Moderate |
| Mometasone furoate | 15-20% | 100-400 mcg | Moderate |
| Ciclesonide | 2-3% | 80-320 mcg | Low |
| Beclomethasone dipropionate | 15-25% | 200-800 mcg | Moderate |
Ciclesonide stands out. It’s designed to stay inactive until it reaches your lungs, then it turns into its active form. That means almost none of it enters your bloodstream. Studies show it has a 3.2 times wider safety margin than fluticasone.
If you’ve been on fluticasone for years and are experiencing side effects, talk to your doctor about switching. You might get the same asthma control with far fewer problems.
How to Use Your Inhaler Right-And Why It Matters
Here’s the truth: if you’re not using your inhaler correctly, you’re wasting most of your dose-and increasing your side effects.
With a pressurized inhaler (pMDI), only 10-20% of the medicine actually reaches your lungs. The rest sticks to your tongue, throat, or falls out of your mouth. That’s why you get thrush and hoarseness.
The fix? Use a spacer.
A spacer is a tube that attaches to your inhaler. It holds the medicine so you can breathe it in slowly. Studies show it:
- Increases lung delivery from 10-20% to 60-80%
- Reduces throat deposition by 70-80%
- Lowers thrush risk from 38.7% to 14.2%
And it’s not just for kids. Adults benefit just as much. Yet, many doctors don’t teach it. One study found that 72% of patients with side effects had never been shown how to use a spacer properly.
Here’s the simple routine:
- Shake your inhaler.
- Attach it to the spacer.
- Breathe out fully.
- Press the inhaler once to release the dose into the spacer.
- Breathe in slowly through your mouth for 4-5 seconds.
- Hold your breath for 10 seconds.
- Wait 30 seconds, then repeat if you need a second puff.
- Immediately rinse your mouth with water and spit it out. Don’t swallow.
That rinse-and-spit step alone cuts thrush risk by half. And it takes 10 seconds. Do it every time.
How to Know If You’re on Too Much
Doctors often start patients on a standard dose. But asthma control isn’t one-size-fits-all. Many people are on more than they need.
GINA guidelines say: use the lowest dose that keeps your asthma under control. That means regular check-ins to see if you can step down.
Ask yourself:
- Have you had fewer flare-ups in the last 6 months?
- Do you use your rescue inhaler less than twice a week?
- Are you sleeping through the night without coughing?
If you answered yes to all three, you might be ready to lower your dose. But don’t do it on your own. Work with your doctor. A 2022 GINA report found that properly managed dose reductions prevented 65-75% of systemic side effects.
For example, if you’re on 500 mcg of fluticasone daily and your asthma is stable, your doctor might try dropping you to 250 mcg. Many people stay controlled at that level.
And if you’re on over 800 mcg of beclomethasone equivalent (about 400 mcg fluticasone), you’re in the high-dose range. That’s when monitoring becomes critical.
Who Needs Extra Monitoring?
Some people are at higher risk-and need more frequent check-ups.
Children: Standard doses cause a tiny growth delay-about 0.7 cm per year. But high doses (>800 mcg) increase cataract risk by more than double. Kids on ICS should have annual eye checks.
Adults over 65: Your bones and lungs are more vulnerable. High-dose ICS raises fracture risk by 31% and pneumonia risk by nearly 70%. Annual bone density scans and pneumonia vaccines are recommended.
Pregnant women: Budesonide is the safest choice. It’s been studied in over 15 years of pregnancy registries. Fluticasone doesn’t have the same safety track record.
People on long-term high doses: If you’ve been on more than 750 mcg/day for over 5 years, get a bone density test. If you’re tired all the time, have low blood pressure, or feel dizzy when standing, ask for a salivary cortisol test. It’s a simple way to check if your adrenal glands are still working properly.

What’s Next? New Options and Hope on the Horizon
The future of asthma treatment is moving away from steroids. Biologics like dupilumab and mepolizumab target specific parts of the immune system that drive inflammation. In trials, they’ve allowed patients to cut their ICS dose by 70% without losing control.
Smart inhalers are also changing the game. These devices track whether you’re using your inhaler correctly and how often. They send alerts to your phone or your doctor if you’re missing doses or using poor technique. One study showed they improve technique accuracy by 92%.
Even newer ICS drugs are in development. AZD7594, for example, showed 90% less adrenal suppression than fluticasone in early trials. These won’t be available everywhere yet, but they’re coming.
The goal isn’t to eliminate steroids overnight. It’s to use them as safely as possible-until better options become standard.
Bottom Line: You Can Manage This
Asthma steroids save lives. But they’re not harmless. The side effects are real, but they’re not inevitable.
Here’s your action plan:
- Use a spacer with every puff.
- Rinse and spit after every use.
- Ask your doctor if you’re on the lowest effective dose.
- Get checked for thrush, voice changes, and bruising every 6 months.
- Consider switching to a lower-absorption steroid like ciclesonide or budesonide.
- Don’t stop your inhaler-even if you feel fine. Stopping suddenly can trigger a dangerous flare-up.
Most people who follow these steps see their side effects drop by half-or disappear entirely. You don’t have to choose between breathing well and feeling bad. You can have both. You just need to use your medicine the right way.





Use a spacer. Seriously. I used to get thrush every other month until my nurse showed me how. Now I rinse, spit, and use a spacer-no more yeast infections. It’s that simple.
Let’s be real-most doctors treat inhalers like they’re candy dispensers. They hand you fluticasone like it’s a free sample at Costco and never mention the spacer. I’ve been on it for seven years. My voice sounds like a broken kazoo. I only found out about ciclesonide because I read a paper on PubMed. Why isn’t this common knowledge?
And don’t get me started on the ‘just rinse your mouth’ advice. Rinsing without spitting is like washing your hands and then licking them. It’s performative hygiene.
The systemic absorption data is rock solid. Fluticasone is basically a slow-burn endocrine disruptor if you’re not monitoring. Budesonide’s 10-15% absorption? That’s the gold standard. Ciclesonide’s 2-3%? That’s the future. Why are we still prescribing the worst option like it’s default?
And yes, I know GINA says ‘lowest effective dose.’ But most primary care docs don’t even know what a GINA guideline is. They just refill the script. I had to bring my own dosing chart to my last appointment.
Also, the pneumonia risk in seniors isn’t ‘nearly 70%’-it’s catastrophic. My aunt died from steroid-induced pneumonia at 71. She was on 500 mcg fluticasone daily. No one warned her. No one even asked if she’d had a flu shot.
Stop treating asthma like a one-size-fits-all condition. This isn’t just medical advice-it’s a systemic failure in patient education.
Oh honey, you’re not wrong-but you’re also not the first person to notice that doctors treat inhalers like they’re magic wands.
I used to be the person who thought ‘rinse and spit’ was a suggestion. Then I started getting thrush so bad I couldn’t eat spicy food. My dentist looked at me like I’d been living in a cave. Turns out, I was just using my inhaler like a toddler with a spray bottle.
Spacers? Game-changer. Like upgrading from a flip phone to an iPhone. Suddenly, I’m getting 80% of the drug where it’s supposed to go. My voice doesn’t sound like a foghorn anymore. My throat doesn’t feel like I gargled with sandpaper.
And ciclesonide? It’s the quiet assassin of inhalers. Doesn’t scream for attention, but it gets the job done without wrecking your insides. If your doctor gives you fluticasone like it’s the only option, ask them why they’re still using the 2008 version of asthma care.
I mean, we have smart inhalers now that text you if you forget to use it. But somehow, we still live in a world where 72% of patients have no idea what a spacer is.
It’s not that we’re bad patients. It’s that the system’s broken. And nobody’s fixing it. So we fix it ourselves. With spacers. And spit. And sarcasm.
lol fluticasone is the worst. u r all just scared of side effects. i had thrush. big deal. i used mouthwash. done. stop overthinking.
also pneumonia? so? old people die. its called aging. stop making asthma sound like a death sentence.
While I appreciate the clinical rigor of this post, I must insist that the omission of any mention of the psychological burden associated with chronic steroid use is a glaring oversight. The emotional toll of managing not just asthma, but the fear of side effects, the ritual of spitting, the shame of hoarseness-it is not merely a physiological condition, but a profound existential recalibration.
Moreover, the suggestion to switch to ciclesonide without acknowledging the accessibility barriers-insurance denials, pharmacy stock shortages, and the sheer bureaucratic inertia of formulary changes-is, frankly, tone-deaf.
And yet… I still use my spacer. Every. Single. Time.
This was so helpful. I’ve been on fluticasone for 10 years and never knew about the spacer. I just thought my voice was getting raspy because I was aging. Thank you for breaking it down so clearly. I’m going to talk to my doctor tomorrow.
Okay, but why is no one talking about the fact that we’re being told to ‘rinse and spit’ like it’s a chore, when the real issue is that these inhalers are designed to be inefficient? Why isn’t the industry being pushed to make better delivery systems? Why are we still using 1980s tech?
I get that spacers help-but they’re clunky. You need to carry them. You need to clean them. You need to remember them. It’s not just patient error-it’s bad design.
And yet, we’re told to adapt. To be more disciplined. To rinse more. To spit harder. But what if the medicine itself was built to not stick to your throat in the first place?
Ciclesonide is a step. But it’s still a band-aid. What about inhalers that only activate when you inhale just right? What about AI-driven dosing that adjusts based on your lung function? Why are we still stuck in the analog age of asthma care?
I’m not mad. I’m just… disappointed.
Let me correct this misinformation: the claim that ciclesonide has a '3.2 times wider safety margin' than fluticasone is not supported by any FDA-approved label or Cochrane review. It is a manufacturer-funded study with a tiny sample size and no long-term outcomes. This post reads like an advertisement disguised as medical advice.
Furthermore, the assertion that '72% of patients have never been shown how to use a spacer' is a gross misrepresentation of the data. The original study cited was conducted in a single urban clinic with non-adherent patients-hardly representative of primary care nationwide.
And while I applaud the effort, this post dangerously undermines physician autonomy by implying that patients should self-prescribe drug switches based on internet research. That’s how people end up on Reddit-sourced biologics and end up in the ER.
Bottom line: trust your doctor. Don’t let a blog post with a table convince you to stop your medication.
Wait-so you’re telling me I’ve been using my inhaler wrong for 12 years? And now you want me to buy a plastic tube and spit out water like I’m a vampire who just drank a smoothie? I’m not doing that. I’ve survived this long. I’m not changing now.
Also, I don’t care if fluticasone is ‘high risk.’ I’m not a lab rat. I’m not getting my cortisol levels tested. I’m breathing. That’s all that matters.
And who the hell is this ‘Sachin Bhorde’ guy? I’ve never heard of him. Is he even a doctor? This whole post feels like a pharmaceutical ad with extra steps.
As a former respiratory therapist, I must say: the spacer advice is 100% correct. But here’s what nobody says: most patients don’t use spacers because they’re embarrassed. They don’t want to look like a child with an inhaler. They think it’s ‘uncool.’
So we need to rebrand it. Call it an ‘aerosol delivery enhancer.’ Or ‘lung optimizer.’ Or ‘asthma pro accessory.’
And for God’s sake, stop calling it a ‘spacer.’ That’s like calling a condom a ‘pregnancy preventer.’ It sounds like a medical device, not a tool of empowerment.
Also, if you’re over 65 and on high-dose ICS, you should be getting bone density scans. Not because you’re old. Because you’re being slowly eroded by your own medication. That’s not aging. That’s iatrogenic decay.
Bro, I'm from India and we don't even have spacers in most clinics. My mom uses fluticasone daily and rinses with water. No spit. No spacer. No doctor visits for 2 years. She's fine. Maybe this is a first-world problem?
Also, ciclesonide costs 3x more than budesonide here. We can't just switch because some American study says so. We need affordable options, not luxury inhalers.
But yeah-rinse and spit. That part I agree with. Even if you're poor, you can do that.
As someone who grew up in a household where asthma meant ‘don’t run, don’t laugh too hard, don’t cry’-this post brought me to tears. Not because it’s sad. Because it’s the first time I’ve seen someone explain this without making me feel broken.
My mother used to tell me, ‘Just breathe through it.’ She didn’t know about spacers. She didn’t know about thrush. She just knew I was wheezing. So she gave me the inhaler and hoped for the best.
Now I use a spacer. I rinse. I spit. I ask my doctor about dose reduction. And I don’t feel guilty for it.
This isn’t just medicine. It’s dignity.
Why are we even talking about this? In America, we have the best healthcare in the world. If you can’t afford a spacer or a new inhaler, you shouldn’t have asthma. Get a better job. Move to a better state. Stop whining.
Also, I’ve been on fluticasone for 15 years. I’ve never had a side effect. So everyone else is just weak. Or lazy. Or both.
SPACER. SPACER. SPACER. I didn’t know what one was until I saw a TikTok about it. Now I carry mine in my pocket like a lucky charm. My voice is back. My throat doesn’t burn. I feel like a new person.
Also, ciclesonide is the real MVP. I switched last year. My doctor was like, ‘Wait, you know about that?’ Yeah. I Googled. And I won.
There is an ethical imperative here that transcends pharmacology: the commodification of health. We are being sold a narrative of individual responsibility-‘rinse and spit’-while systemic failures-lack of provider education, drug pricing, access disparities-are left unaddressed.
The fact that a patient must educate themselves on systemic absorption rates to avoid iatrogenic harm is not a triumph of empowerment. It is a indictment of medical paternalism disguised as autonomy.
And yet, we are told to be grateful for the crumbs of knowledge we find online. To celebrate the spacer as if it were a miracle, when it is merely the bare minimum of competent care.
Let us not mistake survival for justice.
And don’t forget-kids on high-dose ICS need eye exams. My nephew got a cataract at 10. No one told us. Now he needs surgery. Don’t let that be you.