Imagine a medication where the difference between saving your life and harming it is measured in milligrams. This isn't science fiction; it's the reality for patients taking Narrow Therapeutic Index (NTI) drugs, which are medications with a very small margin between effective doses and toxic levels. For most medicines, switching from a brand-name version to a generic is straightforward. But for NTI drugs, that switch can be risky if not managed carefully.
If you or someone you care for takes medications like warfarin, levothyroxine, or tacrolimus, understanding how these drugs work-and why their generic versions require stricter rules-is crucial. The U.S. Food and Drug Administration (FDA) has tightened regulations around these specific drugs because even tiny variations in blood concentration can lead to serious health issues. Let’s break down what makes NTI drugs different, how regulators ensure safety, and what you should watch out for when managing your prescriptions.
What Exactly Are Narrow Therapeutic Index Drugs?
To understand NTI drugs, you first need to grasp the concept of a "therapeutic window." Most drugs have a wide window. If the recommended dose is 100 mg, taking 90 mg or 110 mg usually doesn’t change much. You might feel slightly less relief or a bit more side effect, but nothing catastrophic happens.
NTI drugs do not have this luxury. Their therapeutic window is razor-thin. According to the FDA, these are drugs where "small differences in dose or blood concentration may lead to serious therapeutic failures and/or adverse drug reactions that are life-threatening." In simpler terms, too little of the drug means it doesn’t work (therapeutic failure), and too much means it becomes poisonous (toxicity). There is almost no middle ground.
Common examples include:
- Anticoagulants: Warfarin prevents blood clots. Too little, and you risk a stroke. Too much, and you risk internal bleeding.
- Thyroid Hormones: Levothyroxine manages thyroid function. Small fluctuations can cause severe fatigue, heart palpitations, or metabolic chaos.
- Immunosuppressants: Tacrolimus and cyclosporine prevent organ rejection in transplant patients. Variations can lead to organ loss or severe infection.
- Anti-seizure Medications: Phenytoin and carbamazepine control epilepsy. Instability can trigger seizures or neurological toxicity.
- Antiarrhythmics: Digoxin and flecainide regulate heart rhythm. Toxicity can stop the heart.
As of early 2024, the FDA has officially identified 33 drug products representing 14 distinct active ingredients as NTI drugs. This list continues to grow as newer targeted cancer therapies, such as axitinib and nilotinib, are recognized for their narrow margins.
The Generic Dilemma: Bioequivalence Standards
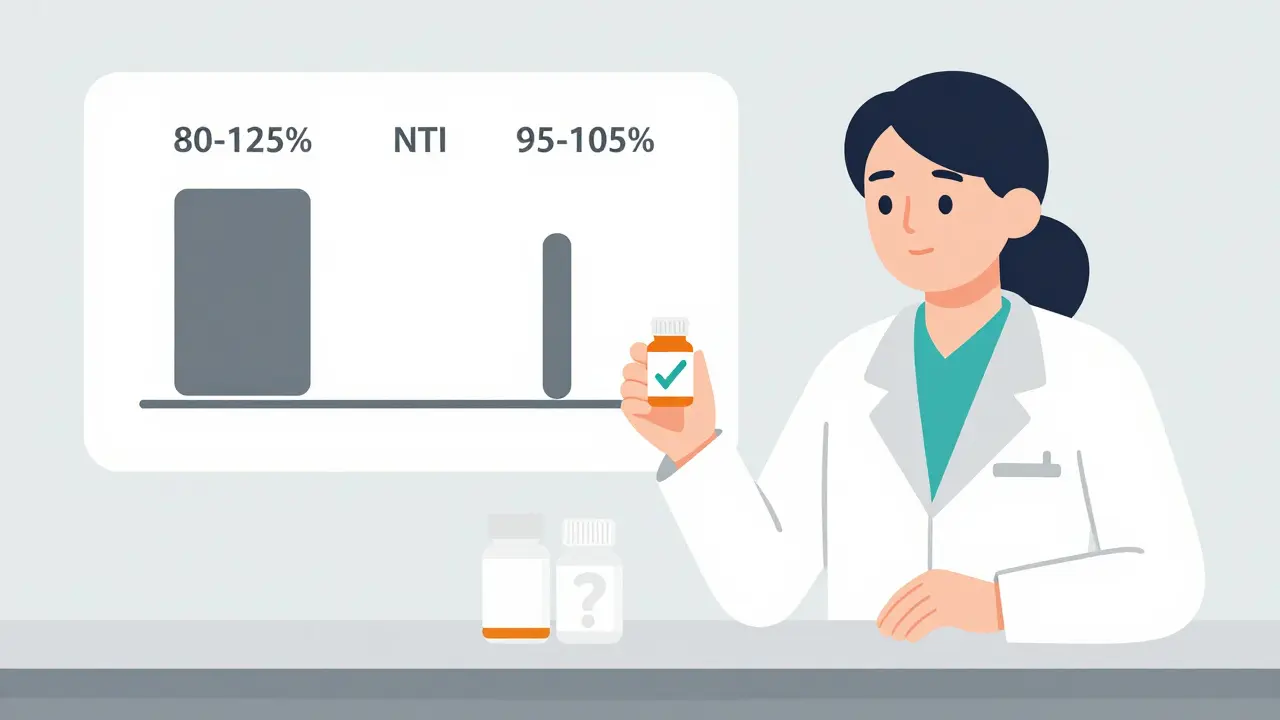
This brings us to the core issue: generics. Generic drugs must be "bioequivalent" to the brand-name original. This means they deliver the same amount of active ingredient into your bloodstream over the same period. For standard drugs, the FDA allows a bioequivalence range of 80% to 125%. If the brand delivers 100 units, the generic can deliver anywhere from 80 to 125 units and still be considered equivalent.
For NTI drugs, this range is far too wide. A 25% variation could push a patient from safe to toxic. Therefore, the FDA enforces much tighter limits for NTI generics:
| Drug Type | Standard Bioequivalence Range | Tightened NTI Range (High Variability) | Tightened NTI Range (Low Variability) |
|---|---|---|---|
| Non-NTI (Standard) | 80% - 125% | N/A | N/A |
| NTI Drugs | Not Applicable | 90% - 111% | 95% - 105% |
When the variability within the reference product is low (around 5%), the generic must match it within 95% to 105%. This ensures that the generic behaves almost identically to the brand. However, achieving this requires more complex manufacturing processes and rigorous testing, which is why fewer companies produce generic NTI drugs compared to standard medications.
Why Pharmacists Hesitate to Substitute
You might wonder why pharmacists don’t just automatically swap brand-name NTI drugs for generics like they do for ibuprofen or amoxicillin. The hesitation comes from real-world clinical experience. A national survey revealed that only 28% of pharmacists were willing to substitute generic versions for initial NTI prescriptions, compared to 78% for non-NTI drugs.
Why the caution? Because individual bodies react differently. Even if two pills are statistically bioequivalent, a specific patient might metabolize one manufacturer’s version slightly faster than another’s. For a standard drug, this doesn’t matter. For an NTI drug, it can.
Consider levothyroxine. Many patients report wild swings in TSH (thyroid-stimulating hormone) levels after switching manufacturers. One pharmacist shared on a professional forum, "I've seen patients on levothyroxine have TSH levels swing wildly after generic substitution, requiring multiple dose adjustments." Similarly, transplant recipients have reported kidney function deterioration (elevated creatinine) after being switched from brand-name Prograf (tacrolimus) to a generic, sometimes requiring hospitalization.
This doesn’t mean generics are bad. It means consistency is key. Once a patient is stable on a specific manufacturer’s product-whether brand or generic-switching them unnecessarily introduces risk.
Regulatory Safeguards and State Laws
Recognizing these risks, regulators have stepped up. The FDA formed the NTI Drug Working Group in 2015 to create consistent criteria. Today, the agency issues Product-Specific Guidances (PSGs) for many NTI drugs, outlining exactly how generics must be tested. Some of these tests use "replicate design studies," which are more complex statistical analyses that look at variability within individuals, not just across groups.
At the state level, laws vary. As of 2023, 42 U.S. states have laws restricting the automatic substitution of NTI drugs. These laws often allow pharmacists to substitute only if the prescriber agrees or if no other option exists. In some states, doctors can write "Dispense as Written" (DAW) on the prescription to prevent any substitution. This is common practice for NTI drugs once a patient is stabilized.
The Joint Commission also mandates strict documentation for NTI medications, requiring therapeutic drug monitoring (TDM) records to ensure blood levels remain within the safe zone. This extra paperwork is a burden, but it’s a necessary safeguard for patient safety.
Practical Tips for Patients and Caregivers
If you take an NTI drug, you are part of a vulnerable population that needs extra attention. Here is how to manage your therapy safely:
- Know Your Drug: Ask your doctor or pharmacist if your medication is classified as NTI. Common ones include warfarin, levothyroxine, phenytoin, carbamazepine, tacrolimus, cyclosporine, and digoxin.
- Monitor Blood Levels: Do not skip therapeutic drug monitoring. Regular blood tests check if your drug levels are in the therapeutic window. For warfarin, this is the INR test. For levothyroxine, it’s TSH. For immunosuppressants, it’s trough levels.
- Stick to One Manufacturer: If you are stable on a specific generic brand (look at the NDC number on the bottle), ask your pharmacy to keep you on that same manufacturer. Consistency reduces the risk of fluctuation.
- Communicate Changes: If your pharmacy switches suppliers, notify your doctor immediately. You may need a blood test sooner than usual to check for changes.
- Don’t Stop Abruptly: Never stop taking an NTI drug without medical supervision. Withdrawal or sudden cessation can be dangerous, especially for anti-seizure or heart medications.
The Future of NTI Drug Management
The landscape of NTI drugs is evolving. The market for these drugs is projected to reach $185.7 billion by 2027, driven largely by new biologics and targeted cancer therapies. Many of these newer drugs have narrow therapeutic indices due to their precise mechanism of action.
One promising development is pharmacogenomics-the study of how your genes affect your response to drugs. By 2028, analysts predict that 40% of NTI drug prescriptions will incorporate genetic testing. This could personalize dosing, reducing the guesswork and minimizing the risk of toxicity. Instead of relying solely on trial-and-error blood tests, doctors could determine the right dose based on your DNA profile.
Additionally, the FDA plans to issue more product-specific guidances by 2025, focusing on newer oncology agents. This trend toward stricter, product-specific standards reflects a maturation in regulatory science. The goal is clear: maintain the cost-saving benefits of generics while ensuring the safety precision required by NTI drugs.
Is it safe to switch from brand-name to generic NTI drugs?
Yes, but with caution. Generic NTI drugs meet stricter bioequivalence standards (90-111% or 95-105%) than regular generics. However, because the therapeutic window is so narrow, some patients may experience fluctuations in blood levels when switching. It is best to switch under medical supervision and monitor blood levels closely afterward. Once stable on a generic, try to stay with the same manufacturer.
How do I know if my medication is a Narrow Therapeutic Index drug?
You can ask your pharmacist or doctor. Common NTI drugs include warfarin, levothyroxine, phenytoin, carbamazepine, tacrolimus, cyclosporine, digoxin, and flecainide. If your medication requires regular blood tests to check its level in your body, it is likely an NTI drug.
Why are bioequivalence standards tighter for NTI drugs?
Standard drugs allow an 80-125% variance in absorption because their therapeutic window is wide. NTI drugs have a minimal margin between efficacy and toxicity. A small increase in absorption could cause poisoning, while a decrease could cause treatment failure. Tighter standards (e.g., 95-105%) ensure the generic performs almost identically to the brand.
Can my pharmacist refuse to substitute a generic for an NTI drug?
In many cases, yes. Depending on state laws and pharmacy policy, pharmacists may hesitate to auto-substitute NTI drugs, especially for new prescriptions. Doctors can also write "Dispense as Written" (DAW) to prevent substitution. This is often done to maintain consistency for patients who are already stable on a specific manufacturer’s product.
What should I do if my pharmacy changes the manufacturer of my NTI drug?
Contact your healthcare provider immediately. Inform them that your medication manufacturer has changed. They may order an earlier-than-scheduled blood test to ensure your drug levels remain within the therapeutic range. Do not stop taking the medication, but be vigilant for any new symptoms.
Are there more NTI drugs being added to the list?
Yes. The FDA continuously reviews drugs for NTI status. Recently, several targeted cancer therapies (like axitinib and nilotinib) have been classified as NTI drugs. The FDA aims to issue more product-specific guidances by 2025 to address newer molecular entities with narrow therapeutic windows.