Psychotropic Medication Weight Gain Risk Checker
Select a medication from the list below or type its name to see its specific weight gain risk profile and average expected weight change.
Medication Name
ClassRecommended Management Strategy:
Why This Matters
Weight gain isn't just about aesthetics. It contributes to metabolic syndrome and heart disease. Early monitoring is key.
Monitoring Guidelines
- Baseline metrics before starting
- Monthly weigh-ins
- Quarterly metabolic checks
- Action if >7% body weight gained
Starting a new prescription for depression, anxiety, or bipolar disorder can feel like finding a lifeline. But there is often a heavy price tag attached to that relief: the scale creeping upward. If you have ever wondered why your waistline expanded despite sticking to your usual diet and exercise routine, you are not imagining it. Psychotropic medications, including antidepressants, antipsychotics, and mood stabilizers, are proven treatments for mental health conditions, but they frequently trigger significant weight gain as a documented side effect.
This isn't just about aesthetics. Weight gain from these drugs contributes directly to metabolic syndrome, heart disease, and a reduced life expectancy. People with severe mental illness already face a 10-to-20-year reduction in lifespan compared to the general population, largely due to medication-induced metabolic complications. The good news? You don't have to accept this outcome as inevitable. With proactive monitoring, strategic medication choices, and targeted lifestyle interventions, you can manage your weight while maintaining your mental stability.
Why Do These Medications Cause Weight Gain?
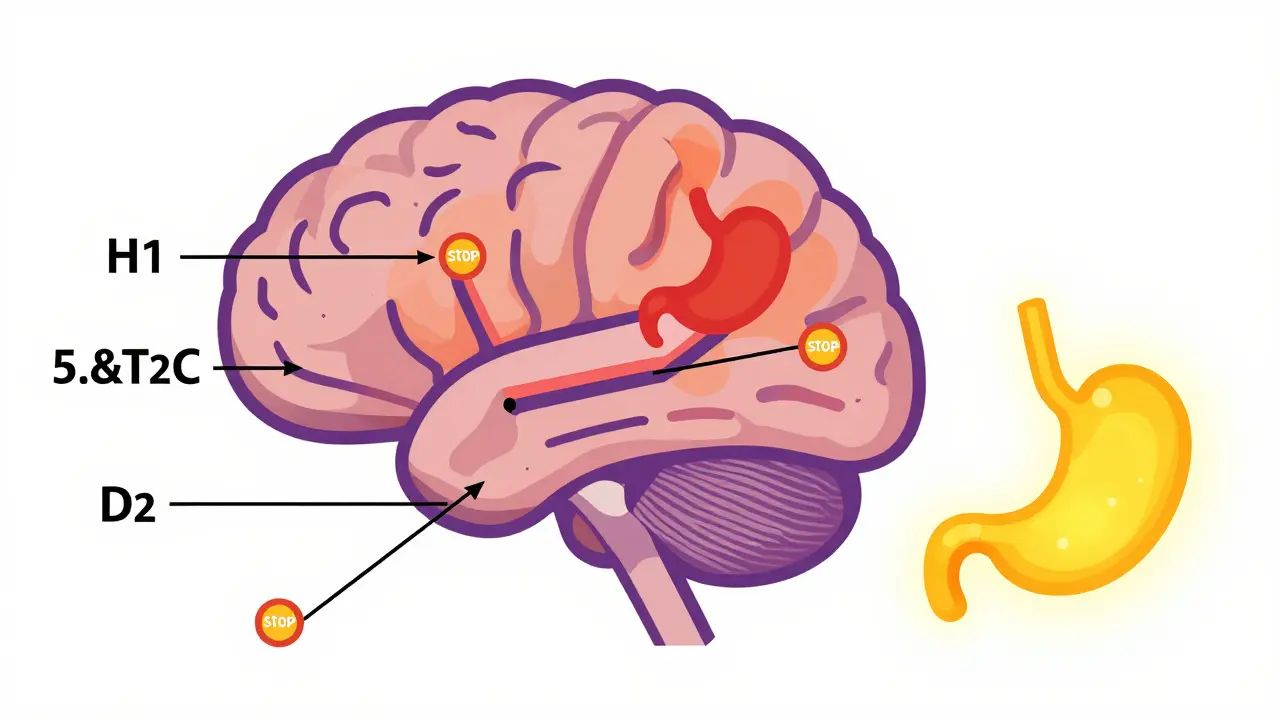
To manage the problem, you first need to understand the mechanism. It’s not simply that you’re eating more because you feel better; although improved appetite plays a role, the biology is deeper. Psychotropic drugs interfere with specific receptors in your brain that regulate hunger, satiety, and metabolism.
The primary culprits are the antagonism of histamine-1 (H1), serotonin-2C (5-HT2C), and dopamine-2 (D2) receptors. When these receptors are blocked, your body signals increased hunger and slows down energy expenditure. For example, blocking H1 receptors mimics the effect of many older antihistamines, making you drowsy and hungry. Blocking 5-HT2C disrupts the signal that tells your brain you’ve had enough to eat. This biological shift creates a state where your body actively resists weight loss, requiring intensified intervention strategies beyond standard dieting.
Not All Meds Are Equal: Risk Profiles by Class
If you are starting treatment or considering a switch, knowing which medications carry the highest risk is crucial. The potential for weight gain varies dramatically between drug classes and even between individual drugs within the same class.
| Medication Class | High Risk Agents | Moderate/Low Risk Agents | Average Weight Change (First Year) |
|---|---|---|---|
| Second-Generation Antipsychotics (SGAs) | Clozapine, Olanzapine | Aripiprazole, Lurasidone, Asenapine | 4-10 kg (High Risk); Minimal (Low Risk) |
| Antidepressants | Mirtazapine, Paroxetine, Amitriptyline | Bupropion, Fluoxetine | Variable; up to 5 kg+ for high risk |
| Mood Stabilizers | Lithium, Valproate | Lamotrigine | Significant for Lithium/Valproate |
Among SGAs, Clozapine and Olanzapine pose the greatest threat. Studies show patients on these drugs can gain an average of 4 kg in just the first 10 weeks, with total gains reaching 10 kg within a year not being uncommon. In contrast, newer agents like Lurasidone and Aripiprazole demonstrate relative metabolic neutrality. Lurasidone, for instance, caused only 0.75 kg of weight gain compared to placebo in clinical trials, a stark difference from olanzapine’s 4.15 kg gain. First-generation antipsychotics like Haloperidol generally cause less weight gain than chlorpromazine, but they come with other neurological risks.
The Biological Resistance to Weight Loss
You might be doing everything right-counting calories, hitting the gym-and still see the needle move the wrong way. This is frustrating, but it is documented science. Research published in PMC6463881 revealed that patients exposed to psychotropic medications lost 1.6% less weight over 12 months compared to those not on these drugs, even when undergoing medical weight management.
Only 31.8% of medicated patients achieved clinically meaningful weight loss (≥10%), compared to 41.2% of unmedicated peers. This "biological resistance" means standard advice like "eat less, move more" is often insufficient. Your body is fighting back against weight loss through hormonal changes, altered glucose metabolism, and increased cholesterol levels. Recognizing this helps remove the shame and guilt. It’s not a failure of willpower; it’s a pharmacological effect that requires a different approach.
Proactive Management Strategies
Waiting until you’ve gained 20 pounds to take action is too late. The American Psychiatric Association guidelines recommend regular monitoring of weight, waist circumference, blood pressure, and metabolic parameters at baseline and quarterly during treatment. Here is how to stay ahead of the curve:
- Baseline Metrics: Before starting a new med, record your weight, BMI, and waist circumference. This gives you a clear reference point.
- Quarterly Check-ins: Don’t wait for your annual physical. Weigh yourself monthly and track trends. A gain of 7% or more of your body weight is considered clinically significant and warrants immediate discussion with your prescriber.
- Dietary Adjustments: Structured meal planning is essential. Since these meds can blunt satiety signals, aim for high-volume, low-calorie foods like leafy greens and lean proteins to keep you full without excess calories. Limit refined sugars, which become more tempting due to dopamine receptor changes.
- Exercise Tailoring: Sedentary behavior is a common side effect. Start small. Even 15 minutes of walking daily can help counteract metabolic slowdown. Focus on consistency rather than intensity initially.
Pharmacological Interventions: Metformin and Beyond
If lifestyle changes aren’t enough, or if you are on a high-risk medication that cannot be switched, adjunctive pharmacotherapy is a valid option. Metformin, commonly used for diabetes, has shown significant efficacy in preventing or reversing antipsychotic-induced weight gain. Multiple randomized controlled trials indicate it can reduce weight gain by approximately 2-4 kg compared to placebo. It works by improving insulin sensitivity and reducing hepatic glucose production.
Another option is Topiramate, an anti-seizure medication that also suppresses appetite. Meta-analyses suggest it can lead to a 3-5 kg weight reduction in patients experiencing medication-induced gain. However, both options require careful medical supervision due to potential interactions and side effects. Never start these without consulting your psychiatrist and primary care provider.
The Future: Precision Medicine and New Tools
We are moving toward a more personalized approach. Researchers are identifying genetic markers, such as polymorphisms in the MC4R gene, that predict who is most susceptible to weight gain. This could soon allow doctors to prescribe based on your genetic profile rather than trial and error.
Emerging therapies include GLP-1 receptor agonists (like semaglutide), originally developed for diabetes, which have shown 5-8% weight reduction in preliminary trials with psychiatric patients. Digital health tools are also gaining traction. Apps like Moodivator, FDA-cleared in 2021, combine behavioral counseling with tracking, demonstrating additional weight loss compared to standard care. These tools offer support between appointments, helping you stay accountable when motivation wanes.
Can I lose weight while staying on my current psychotropic medication?
Yes, but it may require more effort than usual due to biological resistance. Combining structured diet, consistent exercise, and potentially adjunctive medications like metformin can help. Consult your doctor before making any changes.
Which antipsychotic is least likely to cause weight gain?
Aripiprazole, lurasidone, and asenapine are generally associated with minimal weight gain compared to clozapine or olanzapine. However, individual responses vary, so discuss your specific needs with your psychiatrist.
How quickly does weight gain typically occur after starting medication?
For high-risk medications like olanzapine, significant weight gain can begin within the first 10 weeks, averaging 4 kg. Most of the gain occurs in the first year of treatment.
Is metformin safe to use for weight management in psychiatric patients?
Metformin is widely studied and generally safe, but it must be prescribed by a healthcare provider. It has been shown to prevent or reverse weight gain by 2-4 kg in some patients taking antipsychotics.
What should I do if I’ve already gained significant weight?
Don’t stop your medication abruptly. Work with your doctor to explore switching to a lower-risk alternative, adding metformin or topiramate, or intensifying lifestyle interventions. Early detection of metabolic issues is key.